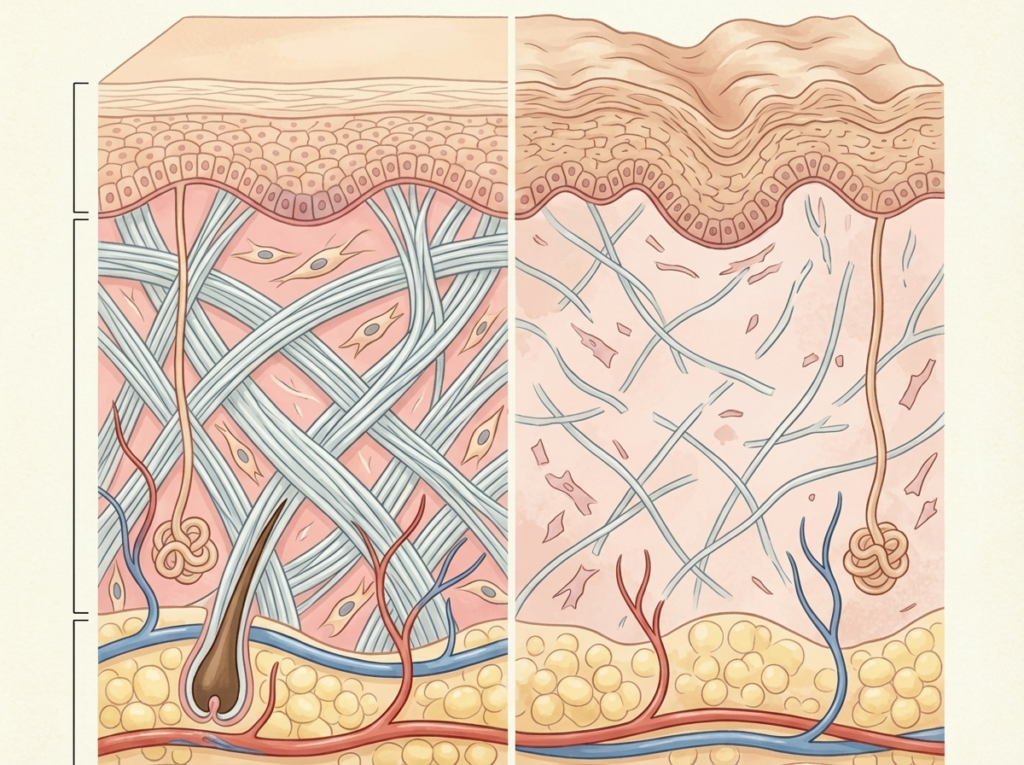
Collagen is the most abundant structural protein in the dermis, accounting for roughly 70 percent of its dry weight. Collagen loss is the single largest contributor to visible skin aging: loss of firmness, increased laxity, deepening of lines, and changes in skin texture. The rate and pattern of this decline are well-characterized in dermatological research, and the data tells a far more specific story than the beauty industry’s generic “anti-aging” messaging typically communicates.
The production curve
Dermal collagen production peaks between ages 20 and 25, when fibroblast density and synthetic activity are at their highest. From this peak, production declines at a rate measured through multiple methodologies: serial biopsies with histological analysis, non-invasive imaging (high-frequency ultrasound, optical coherence tomography), and mechanical testing (cutometry, durometry).
The consensus from this body of evidence establishes an annual collagen loss rate of approximately 1.0 to 1.5 percent from age 25 onward. This rate is not uniform across all individuals and is modulated by genetics, UV exposure history, hormonal status, and lifestyle factors. But the baseline trajectory is consistent across populations.
Cumulative impact by decade
Age 25 to 30: Cumulative decline of 5 to 8 percent. Not visible to most people. The skin retains sufficient structural reserve that the loss is mechanically compensated. This is the decade where prevention strategies (photoprotection, antioxidants) have their highest long-term impact.
Age 30 to 40: Cumulative decline of 10 to 20 percent. The first visible changes typically appear in the mid-to-late thirties: fine lines around the eyes, subtle loss of cheek volume, early changes in skin texture. Elastin fragmentation begins to compound the collagen loss, reducing the skin’s ability to snap back after deformation.
Age 40 to 50: Cumulative decline of 20 to 35 percent. Structural changes become unambiguously visible during this decade. Jawline definition softens, nasolabial folds deepen, and the midface begins to descend as the dermal scaffold weakens. For women, this decade frequently includes perimenopause and the onset of estrogen-mediated acceleration of collagen loss.
Age 50 to 60: Cumulative decline of 35 to 50 percent. In post-menopausal women, the decline accelerates. Research by Brincat et al. documented a 2.1 percent annual decline in skin collagen content in the years immediately following menopause, roughly double the pre-menopausal rate. Up to 30 percent of dermal collagen can be lost in the first five post-menopausal years alone.
Age 60 and beyond: Cumulative decline of 50 to 65 percent from peak. The dermal scaffold is substantially thinned. Mechanical testing shows measurable reductions in skin tensile strength and elastic recovery time.

The estrogen factor
Estrogen’s role in collagen maintenance is distinct from and additive to the age-related collagen loss. Estrogen receptors on fibroblasts modulate collagen synthesis. Declining estrogen levels during perimenopause and menopause directly reduce fibroblast synthetic activity, creating an acceleration event layered on top of the gradual age-related decline.
This acceleration is clinically relevant. A woman at 45 with normal estrogen levels and a woman at 45 in early menopause may have materially different collagen densities despite identical chronological age. The hormonal variable explains much of the inter-individual variation observed in skin aging among women of the same age.
Hormone replacement therapy (HRT) has been shown to partially mitigate the menopausal acceleration of collagen loss, though this is a medical decision with considerations beyond dermatological benefit. The relevant point for skin health is that hormonal status is a meaningful modifier of the collagen decline rate.
UV exposure: the dominant external variable
Intrinsic aging (the genetic and hormonal factors described above) accounts for one dimension of collagen loss. Photoaging, the damage caused by cumulative UV exposure, represents a parallel and often dominant pathway.
UV radiation activates matrix metalloproteinases (MMPs), enzymes that actively degrade collagen and elastin in the dermis. In chronically sun-exposed skin, MMP-mediated degradation can exceed the rate of new collagen synthesis even in younger individuals, producing premature structural aging.
The clinical relevance of photoaging is most visible in sun-protected versus sun-exposed skin on the same individual. The inner upper arm of a 60-year-old typically shows better collagen integrity than the dorsal hand or face of the same person. The biology is identical; the UV exposure history is different.
This comparison makes clear that collagen loss is not solely an inevitable consequence of aging. A substantial portion is environmentally driven and preventable through consistent UV protection.
Intervention efficacy across the collagen loss curve
The effectiveness of interventions that address collagen loss is time-dependent. Earlier intervention produces disproportionately better results because the target tissue (fibroblasts in the dermis) is more responsive to stimulation when the structural scaffold is still relatively intact.
Topical retinoids demonstrate strong evidence for stimulating fibroblast activity and increasing collagen production in the upper dermis. Efficacy is highest in the 30s and 40s, when the fibroblast population is still dense and active. Efficacy diminishes in older skin where fibroblast density has declined, though benefits to epidermal quality persist.
Energy-based treatments (radiofrequency, microneedling, low-level laser therapy, and LED photobiomodulation) trigger neocollagenesis (the body’s process of building fresh collagen) through controlled energy delivery to the dermis. Clinical-grade and consumer-grade systems access the same biological mechanism at different intensities. The compound effect of consistent treatment over years produces cumulative structural improvement that single-session approaches cannot match.
Photoprotection is the single highest-efficacy intervention across all decades by a wide margin, because it prevents collagen degradation rather than attempting to rebuild it. The return on investment from daily sunscreen use exceeds any regenerative modality, though it is complementary rather than competitive with active collagen-building treatments.
Each treatment cycle for collagen rebuilding takes approximately 60 to 90 days from stimulus to mature collagen. Consistent treatment over years produces cumulative gains that exceed what any single intervention cycle can deliver. A woman who begins a consistent collagen-stimulating protocol at 35 and maintains it through her 40s enters the menopausal acceleration event with a structurally stronger dermis than she would have without intervention. The collagen built during her 30s provides a buffer against the accelerated loss of her 50s.
A woman who begins the same protocol at 55 is working against a reduced fibroblast population and an already-thinned collagen scaffold. The intervention still produces benefit, but the absolute structural gain per cycle is lower.
This temporal dynamic argues for earlier, less intensive, consistent intervention over later, more aggressive, corrective intervention. Prevention and early building produce outsized long-term returns.
Practical implications
The collagen loss curve is not destiny. It is a framework for informed decision-making.
For consumers, the decision points are clear: begin photoprotection immediately (age-independent), introduce a retinoid in the late 20s or early 30s, consider energy-based collagen stimulation in the mid-30s and beyond, and maintain these interventions as ongoing protocols rather than intermittent purchases.
For practitioners, the data supports proactive collagen-health counseling beginning in the 30s, with protocol adjustment through each decade based on the patient’s specific collagen status (assessable through cutometry, ultrasound imaging, or clinical observation).
The biology is specific, measurable, and well-characterized. The interventions with evidence of efficacy exist and are accessible. The remaining gap is awareness: most consumers encounter collagen decline data only after structural changes have become visible, when the most cost-effective intervention window has already partially closed.