There is a particular frustration built into aesthetic treatments that rely on the skin’s own biology to produce results. The treatment itself takes minutes. The biological response takes weeks. And during those weeks, the mirror offers little encouragement.
This is not a flaw in the treatment. It is a feature of the biology. Skin collagen remodeling follows a well-characterized sequence that begins within hours of a stimulus and unfolds over 60 to 90 days before producing changes visible to the human eye. Understanding what is happening at each stage makes the difference between abandoning a protocol that was working and staying with it long enough to see the outcome.
The three-phase biological response
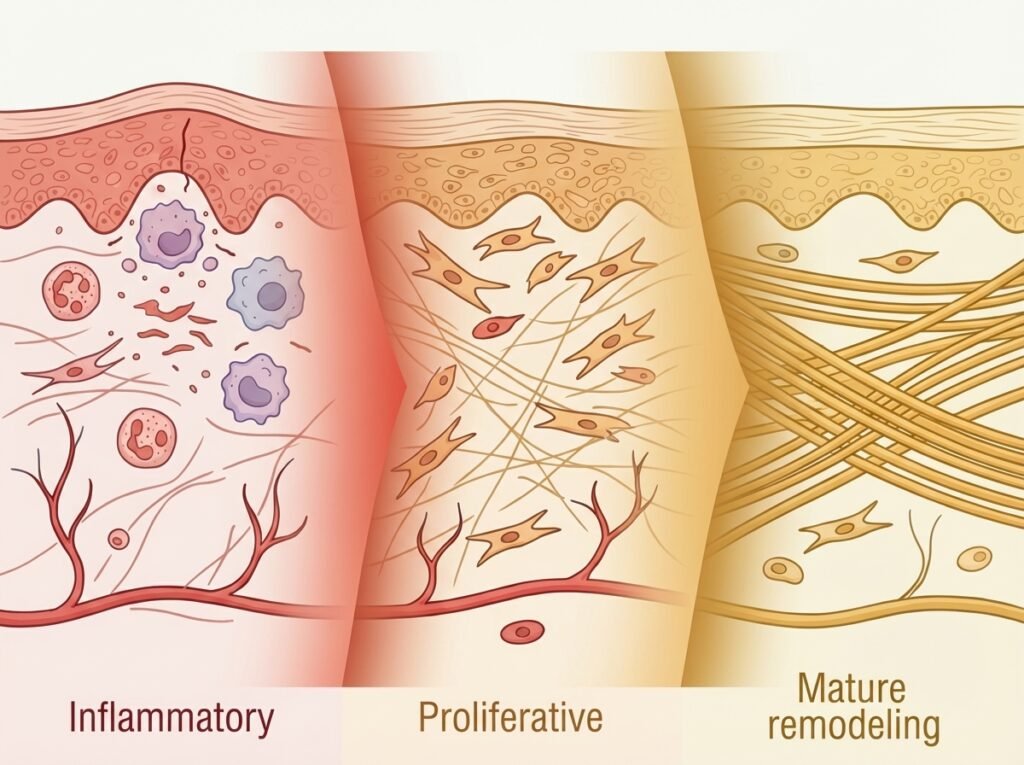
Every energy-based aesthetic treatment (radiofrequency, microneedling, LED, fractional laser) triggers some version of the same biological cascade. The wound healing literature describes three overlapping phases: the inflammatory phase, the proliferative phase, and the remodeling phase. In aesthetic contexts, the “wound” is deliberately mild, a controlled micro-stimulus rather than an injury, but the cellular response follows the same sequence.
Week 1 to 2: the inflammatory phase
The body’s first response to controlled energy delivery is an inflammatory cascade. Growth factors and cytokines flood the treated area, recruiting immune cells and signaling fibroblasts that repair work is needed.
What the mirror shows: potentially nothing, or a slight flush, minor texture change, or temporary sensitivity. The skin may actually look marginally worse for a few days after certain modalities (microneedling in particular). This is normal. It is the biological equivalent of a construction crew arriving at a site before any building has started.
This phase is quick, typically resolving within 5 to 7 days. Its purpose is signaling, not construction.
Week 2 to 4: the proliferative phase
Fibroblasts, the cells responsible for producing collagen and elastin, migrate to the treatment zone and begin synthesizing new structural protein. The collagen being produced at this stage is predominantly Type III collagen, a thinner, more flexible form that serves as scaffolding for the stronger collagen that will follow.
What the mirror shows: almost nothing. Type III collagen is structurally present but not yet dense enough to change the skin’s visible firmness or texture. The skin may feel slightly smoother to the touch, but the change is subtle enough that most people would not notice it without being told to look for it.
This is the phase where abandonment begins. The treatment sessions require effort (time, consistency, discipline), the biological response is real and measurable, and the visible return is minimal. The gap between effort and reward is at its widest.
Week 4 to 8: the remodeling phase
The remodeling phase is where the biology does its most important work. Type III collagen is progressively cross-linked and replaced by Type I collagen, a thicker, more structurally rigid form that accounts for roughly 80 percent of collagen in mature adult skin. Lysyl oxidase, an enzyme that catalyzes covalent bonding between collagen molecules, strengthens the new fibers into a load-bearing network.
What the mirror shows: the earliest hints of visible change, but still below the threshold of what most people recognize as a “result.” Skin may feel firmer when pressed. Fine lines may appear marginally softer. The improvement is real, but incremental enough to be dismissed as imagination.
This is the peak abandonment window. The treatment has been running for over a month. The biology, if measured by cutometry (a device that quantifies skin firmness) or high-frequency ultrasound, shows clear structural improvement. The eye, however, is not a precision instrument, and the change has not yet accumulated to the point of obvious visual difference.
Week 8 to 12: the visibility threshold
Skin collagen remodeling reaches a critical mass somewhere in this window. Cumulative Type I collagen density crosses the threshold where mechanical properties (firmness, elasticity, bounce-back speed) produce visible change under normal lighting and observation conditions.
What the mirror shows: the result. This is the point where the reflection starts to look different. Skin appears firmer, lines look softer, texture is smoother. The change feels sudden, even though the biology has been building toward it for weeks.
A randomized, placebo-controlled study of LED phototherapy by Lee et al. documented this pattern precisely: treatments delivered twice weekly for four weeks produced measurable collagen and elastic fiber increases histologically, with peak visible improvement (up to 36 percent wrinkle reduction and 19 percent elasticity increase) continuing to develop for three months after the treatment series.
Cumulative sessions compound the response
Each treatment session restarts the three-phase cascade. When sessions are spaced appropriately (the biology determines the interval, not the calendar), multiple overlapping cycles create a compounding effect.
Session 1 initiates Cycle 1. By the time Cycle 1 reaches remodeling (week 4), Session 5 or 6 has initiated new cycles that are now in their proliferative phase. The skin is simultaneously building new collagen from multiple stimuli at different stages of maturation.
Over 12 weeks of consistent treatment, the collagen density curve steepens with each passing week because earlier cycles are depositing mature Type I collagen while later cycles are building the Type III scaffolding that will become the next wave of mature collagen. The result is a cumulative structural gain that no single treatment session could produce on its own.
The measurement gap
The frustrating irony is that tools exist to detect the biological changes long before the mirror does.
Cutometry, which measures skin firmness by applying suction and measuring the deformation response, can detect significant improvement as early as week 4. High-frequency ultrasound can visualize increased dermal density at a similar stage. Clinical photographers using standardized conditions can identify subtle improvements that casual observation misses.
Consumers have access to none of these tools. The measurement instrument available at home is the mirror, and the mirror is the least sensitive detector of the changes that energy-based treatments produce. This mismatch, between what is biologically present and what is visually apparent, is the single largest driver of premature protocol abandonment.
The biology makes a strong case for patience, but patience is easier to sustain with understanding. Knowing that the skin is actively building collagen during weeks 4 through 8, even though the mirror shows nothing dramatic, reframes the experience from “this isn’t working” to “this is in progress.”